-
Reviewed
For the most up to date information on this topic, please visit jeanhailes.org.au
Key takeaways
- Common symptoms of adenomyosis include painful and heavy periods, and pelvic pain.
- Adenomyosis is different to endometriosis, but you can have both conditions at the same time.
- Treatments include hormone medicines and surgery.
- See your doctor if symptoms like painful periods impact your daily life.
Key takeaways
- Common symptoms of adenomyosis include painful and heavy periods, and pelvic pain.
- Adenomyosis is different to endometriosis, but you can have both conditions at the same time.
- Treatments include hormone medicines and surgery.
- See your doctor if symptoms like painful periods impact your daily life.
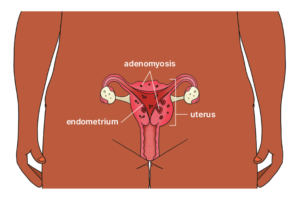
What is adenomyosis?
Adenomyosis is a condition where tissue, similar to the lining of the uterus, grows into the muscle wall of the uterus.
In the past it was thought that adenomyosis mainly affected women aged 40 to 49 years, but it’s now clear that the condition can also affect younger women (including teens).
Women with adenomyosis can often have endometriosis too, but the conditions are different. With endometriosis, the tissue grows in other parts of your body, such as your fallopian tubes and ovaries.
How can adenomyosis affect periods?
Adenomyosis can cause the uterus to thicken and enlarge, sometimes resulting in heavy or long periods and pain.
How can adenomyosis affect fertility?
Adenomyosis can cause fertility problems because the condition makes it harder for:
- sperm to fertilise an egg
- embryos to implant into the lining of the uterus
- embryos to develop.
Women with adenomyosis also have a higher chance of pregnancy complications, such as miscarriage. Ask your doctor for more information.
Symptoms of adenomyosis
Adenomyosis affects each woman differently. About one in 3 women don’t experience any symptoms.
For women who do experience symptoms, they usually include:
- painful periods
- heavy periods
- longer menstrual cycles
- iron deficiency (anaemia) due to heavy periods, which can make you feel tired or dizzy
- painful sex (dyspareunia)
- persistent pelvic pain
- bloating or pressure in your belly
- bleeding or spotting between periods
- blood clots during your periods
- waking at night to wee
- low energy
- lower back pain or pain that goes down the legs
- constipation or diarrhoea.
Causes of adenomyosis
We don’t know the exact cause of adenomyosis, and there could be more than one type. It may be related to:
- injuries to the uterus (e.g. from surgery or childbirth)
- tissue growing in the muscle wall of the uterus before birth
- changes to your body’s immune system (a system that protects you from infections and diseases)
- contact with chemicals that affect your hormones.
How is adenomyosis diagnosed?
Adenomyosis is usually diagnosed by asking about a person’s symptoms, reviewing their medical history and doing a transvaginal ultrasound or MRI to take a picture of the uterus.
Adenomyosis can be hard to diagnose because there are no agreed tests to confirm the condition. Adenomyosis can’t be diagnosed from blood tests or tissue samples (biopsies).
A diagnosis of adenomyosis is usually only confirmed after the uterus has been removed (hysterectomy).
Adenomyosis can sometimes be misdiagnosed as uterine fibroids or endometriosis.
Treatments for adenomyosis
Treatment for adenomyosis will depend on your symptoms, stage of life and whether you plan to have children.
Non-steroidal anti-inflammatory drugs (NSAIDs), for example, ibuprofen, can be used for pain relief, with or without paracetamol.
Hormone treatments may help reduce painful periods and bleeding days. Options include hormonal IUDs, hormone implants, dienogest and the Pill.
The Pill may reduce bleeding and pain, but research suggests it’s not as effective as other hormone treatments.
Talk to your doctor about the benefits and risks of each treatment option.
If you want to become pregnant in the future, you can have surgery to remove abnormal areas of the uterus. This may improve fertility, but it’s important to discuss the risks with your doctor.
If you’re not planning any future pregnancies, you can have an operation to:
- remove the lining of the uterus (endometrial ablation)
- remove the uterus (hysterectomy).
These surgeries stop heavy bleeding during periods and may reduce pain.
A non-surgical procedure called a uterine artery embolisation blocks blood supply to part of the uterus.
This procedure reduces pain and bleeding, but it’s not recommended if you’re planning future pregnancies.
There isn’t enough evidence to show the effectiveness of non-medical treatments for adenomyosis. Some options women use to help manage symptoms include:
- pelvic physiotherapy to help with pelvic pain and pain during sex
- mindfulness, psychological therapy or counselling to improve pelvic pain and quality of life
- acupuncture to improve pain and quality of life
- yoga.
When to see your doctor about adenomyosis
Talk to your doctor if symptoms, such as painful periods, stop you from doing day-to-day activities.
Review process
Our review process
This information has been reviewed by clinical experts and is based on the latest evidence.
Our content review process ensures our health information is accurate, trustworthy, current and useful.
We regularly check our information to make sure it reflects the latest clinical guidelines and key findings from large, reliable studies.
Where possible, we focus on Australian research to make our information more relevant locally.
Experts play a key role in reviewing our content. Clinicians at Jean Hailes check information for accuracy and real‑world relevance. These include GPs, gynaecologists, endocrinologists, psychologists and allied health professionals.
We also work with partner organisations, independent specialists and people with lived experience to make sure our content reflects both expert knowledge and the experiences of the community.