-
Reviewed
For the most up to date information on this topic, please visit jeanhailes.org.au
Key takeaways
- Hysterectomy is a major surgery that cannot be reversed.
- A hysterectomy can impact your health and quality of life, and you will not be able to become pregnant after the surgery.
- It is important to discuss the risks and benefits of hysterectomy carefully with your doctor.
Key takeaways
- Hysterectomy is a major surgery that cannot be reversed.
- A hysterectomy can impact your health and quality of life, and you will not be able to become pregnant after the surgery.
- It is important to discuss the risks and benefits of hysterectomy carefully with your doctor.
What is a hysterectomy?
A hysterectomy is an operation to remove your uterus (womb). There are different types of hysterectomy and related procedures.
If you have a hysterectomy, doctors usually recommend keeping the ovaries, because removing them can cause early menopause and other health issues.
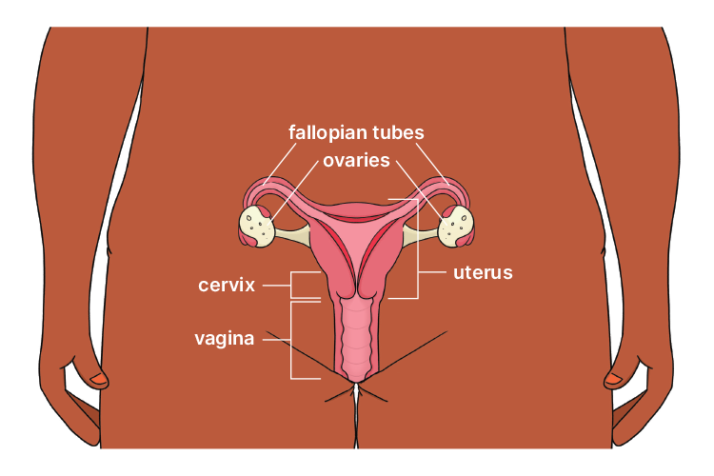
Different types of hysterectomy
A total hysterectomy involves the removal of your uterus and cervix. This is a common procedure, as removal of the whole uterus lowers the risk of future health problems like pain, heavy periods, cancer or fibroids.
A subtotal hysterectomy involves the removal of your uterus, leaving the cervix in place.
An oophorectomy is the removal of the ovaries. This procedure can lower the risk of ovarian cancer.
A salpingectomy is the removal of the fallopian tubes at the same time as a hysterectomy. Most serious ovarian cancers start in the fallopian tubes, so this procedure can lower the risk of developing ovarian cancer.
If you’re considering a hysterectomy, it’s important to understand whether your cervix, ovaries or fallopian tubes will be removed, and why.
Factors that may influence your decision include:
- the reason for the hysterectomy
- your general health
- other medical conditions
- your age
- your cancer risk.
Reasons for having a hysterectomy
Hysterectomy is a major surgery that cannot be reversed. A hysterectomy can impact your health and quality of life, and you will not be able to become pregnant after the surgery.
In most cases, a hysterectomy is only recommended if other treatments have not worked.
The most common reasons for having a hysterectomy are:
- heavy periods
- fibroids
- adenomyosis
- cancer or precancer of your cervix, uterus, ovaries or fallopian tubes.
Your doctor might suggest you consider a hysterectomy for other reasons (for example, endometrial hyperplasia or endometriosis) if you have tried other treatments without success. It is important to discuss the risks and benefits of hysterectomy with your doctor.
Do you need a doctor’s referral for a hysterectomy?
Yes, you will need a doctor’s referral to see a specialist (gynaecologist) who can perform the hysterectomy.
How is a hysterectomy performed?
A hysterectomy can be performed in different ways, depending on:
- the reason for the procedure
- your medical history
- your overall health.
Hysterectomies are usually performed under general anaesthetic.
The main types of hysterectomy procedures are:
- keyhole surgery, performed through small cuts in your belly (laparoscopy)
- surgery via your vagina
- surgery through a cut in your lower belly.
Ask your doctor about the different options and the benefits and risks of each. If you’re still unsure, you can get a second opinion.
What happens after a hysterectomy?
Most women report that their quality of life improves after a hysterectomy. But there are some long-term impacts to be aware of.
It usually takes 2 to 6 weeks for healthy women to recover from a hysterectomy. It can take longer if the operation is more complex, or if there are complications.
To learn more about recovering from a hysterectomy, visit the Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG) website.
You may feel low or depressed after a hysterectomy. This could be due to hormonal changes, or feelings about no longer being able to get pregnant.
Know that you are not alone. Talk to people you trust and see your doctor if you are concerned.
If you have a hysterectomy and keep your ovaries, your periods will stop. But that doesn’t mean you are in menopause.
When both ovaries are removed during surgery, you will experience menopause right away (medically induced menopause).
Talk to your doctor if you have menopausal symptoms after the surgery.
Review process
Our review process
This information has been reviewed by clinical experts and is based on the latest evidence.
Our content review process ensures our health information is accurate, trustworthy, current and useful.
We regularly check our information to make sure it reflects the latest clinical guidelines and key findings from large, reliable studies.
Where possible, we focus on Australian research to make our information more relevant locally.
Experts play a key role in reviewing our content. Clinicians at Jean Hailes check information for accuracy and real‑world relevance. These include GPs, gynaecologists, endocrinologists, psychologists and allied health professionals.
We also work with partner organisations, independent specialists and people with lived experience to make sure our content reflects both expert knowledge and the experiences of the community.