-
Reviewed
For the most up to date information on this topic, please visit jeanhailes.org.au
Key takeaways
- Fibroids are very common in women under the age of 50.
- They can cause heavy periods, painful periods and irregular bleeding.
- If symptoms don’t impact your daily life, you can leave them untreated.
- See your doctor if you have very heavy periods or a sudden change to your bleeding.
Key takeaways
- Fibroids are very common in women under the age of 50.
- They can cause heavy periods, painful periods and irregular bleeding.
- If symptoms don’t impact your daily life, you can leave them untreated.
- See your doctor if you have very heavy periods or a sudden change to your bleeding.
What are fibroids?
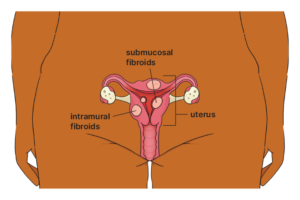
Fibroids are noncancerous growths found in the muscle wall of the uterus. They can vary in size from less than one cm to more than 15 cm in width.
Fibroids can grow:
- on the outer wall of the muscle (subserosal)
- within the muscle wall (intramural)
- on the inner wall lining the cavity of the uterus (submucosal).
Fibroids are common. In Australia, about 7% of women are diagnosed with fibroids by the age of 49, but there are likely many more who have not been diagnosed.
How can fibroids affect fertility?
Some fibroids can cause fertility and pregnancy complications, including:
- difficulty getting pregnant naturally or with IVF
- a higher risk of miscarriage or premature births.
If you have fibroids and are planning a pregnancy, talk to your doctor about treatment options.
Symptoms of fibroids
Fibroids affect each woman differently, partly based on the size, number and position of the fibroids.
After menopause, fibroids usually shrink and symptoms may go away.
About 20% to 30% of women experience some symptoms related to fibroids. Common symptoms include:
- heavy periods or longer periods than normal
- painful periods
- bleeding in between periods – this depends on the size and position of the fibroids
- iron deficiency (anaemia), due to heavy periods, which can make you feel tired or dizzy
- painful sex (dyspareunia)
- feeling heaviness or pressure in your back, bowel or bladder
- feeling like you haven’t emptied your bowel or bladder
- weeing a lot
- swelling in your lower abdomen.
Causes of fibroids
We don’t know exactly what causes fibroids, but we do know the female hormones estrogen and progesterone stimulate the growth of fibroids.
Fibroids may be associated with:
- certain genes
- problems with wound healing
- environmental exposures in early years.
Many risk factors for fibroids can’t be changed, such as:
- your family history
- health conditions like PCOS
- when your first periods started.
But you can work with a doctor to manage risk factors such as weight and blood pressure.
How are fibroids diagnosed?
If you think you have symptoms of fibroids, talk to your doctor. They will ask questions about your symptoms and medical history.
If your doctor suspects fibroids, they should recommend more tests to confirm a diagnosis and help with treatment decisions.
Tests might include:
- an external ultrasound on your belly (abdomen)
- a transvaginal ultrasound to see inside the uterus – this is more accurate than an external ultrasound
- an ultrasound called a saline infusion sonohysterography (SIS), where fluid is put in the uterus to improve the ultrasound picture
- a magnetic resonance imaging (MRI) scan or computed tomography (CT) scan
- a hysteroscopy – a thin telescope shows the inside of your uterus
- a laparoscopy – a thin telescope goes through a small cut in your belly to see your pelvic organs (performed under general anaesthetic).
Treatments for fibroids
Most fibroids don’t need treatment, unless:
- you’re planning to get pregnant
- symptoms stop you from doing things you normally do.
If fibroids don’t affect your daily life, you can choose to leave them untreated.
Medicines are mainly used to reduce bleeding symptoms and pain. Hormone medicines also help to shrink the fibroids.
Your doctor may recommend different medicines to treat your fibroids. For example:
- tranexamic acid tablets
- non-steroidal anti-inflammatory drugs (NSAIDs), such as mefenamic acid tablets
- hormone medicines, such as the Pill, an IUD, elagolix, relugolix, goserelin and nafarelin.
Radiological procedures can be used to treat some fibroids. with radiological treatment. For example:
- uterine artery embolization, a non-surgical procedure that blocks blood supply to part of the uterus
- high-intensity ultrasound, guided by magnetic resonance imaging (MRI).
These treatments aren’t recommended if you want to become pregnant.
You may need surgery to remove your fibroids. The type of surgery will depend on the size and position of your fibroids. Surgery options include:
- a myomectomy to remove fibroids – performed as a hysteroscopy or laparoscopy
- a hysterectomy to remove the uterus.
When to see your doctor about fibroids
See your doctor if you experience one or more symptoms of fibroids.
With treatment, your quality of life is likely to improve.
Review process
Our review process
This information has been reviewed by clinical experts and is based on the latest evidence.
Our content review process ensures our health information is accurate, trustworthy, current and useful.
We regularly check our information to make sure it reflects the latest clinical guidelines and key findings from large, reliable studies.
Where possible, we focus on Australian research to make our information more relevant locally.
Experts play a key role in reviewing our content. Clinicians at Jean Hailes check information for accuracy and real‑world relevance. These include GPs, gynaecologists, endocrinologists, psychologists and allied health professionals.
We also work with partner organisations, independent specialists and people with lived experience to make sure our content reflects both expert knowledge and the experiences of the community.