Menopause can cause a range of physical and emotional changes, such as hot flushes, vaginal changes and mood swings. Every woman will have a different experience.
Physical and emotional symptoms
Hot flushes and night sweats
Sleep disturbance
Mood and emotional health
Bladder, vaginal and vulval problems
Aches and pains
Related resources
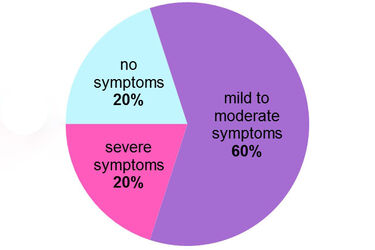
About 20% of women have no symptoms at all, while 60% have mild to moderate symptoms. The remaining 20% have severe symptoms that interfere with their daily life.
Menopausal symptoms can be influenced by different things. For example, your stage of life and general health and wellbeing.
Many symptoms start during perimenopause and can continue into postmenopause. Australian studies show that some women experience symptoms like hot flushes and night sweats well into their 60s.
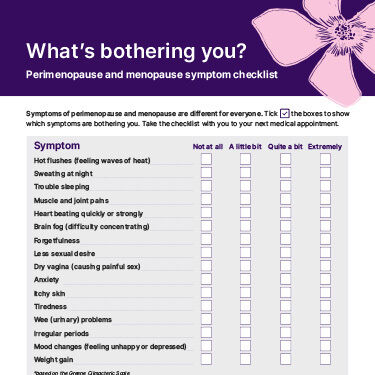
Symptoms of perimenopause and menopause are different for everyone. Tick the boxes to show which symptoms are bothering you. Take the checklist with you to your next medical appointment.
Physical symptoms may include:
Psychological and emotional symptoms may include:
Watch this video of a Jean Hailes endocrinologist talking about menopause and what to expect.
More than 57% of women experience hot flushes and night sweats during menopause. They generally start in your chest area and spread to your upper chest, neck and face. They can also spread over your whole body. The flushes may feel like a burning, overheating sensation. You may also have reddening of the skin and different degrees of sweating. When a flush happens at night, it’s called a night sweat.
Everyone experiences hot flushes differently. For example, you might have mild, quick hot flushes every now and then, or you might have more than 20 a day.
We don’t know exactly what causes hot flushes. Lower oestrogen levels may affect parts of the brain that regulate your body temperature. Many studies suggest that stress and anxiety can influence the frequency and intensity of hot flushes. Some foods or alcohol can also have an impact.
It’s common for your sleep patterns to change during perimenopause and menopause. Around 25% of women aged 50–64 years experience sleep problems. Sleep difficulties are more common after menopause.
Women who have experienced surgical menopause are more likely to report severe symptoms.
Poor sleep can cause other health issues. It has been linked to cardiovascular disease, obesity, mood disorders and diabetes. It is also associated with increased mortality.
Sleep disturbance can be caused by:
Visit the Sleep Health Foundation website for more information about menopause and sleep.
You may notice that menopause causes your mood to change. This is due to changing hormone levels. You might experience:
Research suggests that women are more likely to feel depressed during the menopause transition.
Women who have a history of depression or premenstrual syndrome (PMS) may be more likely to develop depression during this time.
As you move into perimenopause and menopause, low oestrogen levels can change your vulval, vaginal and bladder tissues. These changes may affect up to half of postmenopausal women.
Declining oestrogen levels causes bladder and vaginal tissue to become thin. This can affect areas such as your:
These changes are commonly known as vaginal atrophy.
Around the time of menopause, you might experience vaginal dryness and reduced vaginal elasticity. This can lead to pain during sex and a loss of sex drive (libido).
Learn more about painful sex and treatment options.
You might experience vaginal and vulval irritation during the menopause transition. Typical symptoms include:
Ageing and menopause can cause your pelvic floor muscles to become weaker. Your pelvic floor muscles help you hold your wee in. Menopause also causes your bladder to become less elastic, which means it can’t hold as much wee as it used to. These changes can lead to urinary symptoms such as:
While symptoms such as hot flushes usually disappear over time, bladder, vaginal and vulval problems can persist and may even get worse. But many effective treatments are available.
Changing hormones, particularly a drop in oestrogen levels, can cause aching, painful joints and other musculoskeletal symptoms.
Oestrogen is important for your joint health, as it protects against inflammation. It also helps regulate fluid around your joints.
During menopause, joint pain is commonly experienced in your knees and hips. It may also occur in your shoulders, neck, elbows and hands. Your aches and pains might be stronger in the morning and fade later in the day.
This web page is designed to be informative and educational. It is not intended to provide specific medical advice or replace advice from your health practitioner. The information above is based on current medical knowledge, evidence and practice as at August 2022.
This content has been reviewed by a group of medical subject matter experts, in accordance with Jean Hailes policy.
© Jean Hailes Foundation. All rights reserved. This publication may not be reproduced in whole or in part by any means without written permission of the copyright owner. Contact: licensing@jeanhailes.org.au

